The Best Laid Plans. COVID-19
First published on March 12, 2020
Complete research here: The Best Laid Plans COVID-19
Before I start, I should mention I fall into four of the top five risk categories for COVID-19. I have family who are particularly at risk also. To be blunt, I have skin in the game. But this isn’t about me or you. It is about us all.
Updated June 16th, 2020: Please check out this daily blog being maintained by a Swiss Doctor on what is happening globally. It contains many links to support the below and the comments in the blog. https://swprs.org/a-swiss-doctor-on-covid-19/.
We are currently dealing with the largest global stressor ever experienced in modern history. Note I didn’t say pandemic or crisis. That would have been anything from World War I, II, Spanish Flu or countless other scenarios that have killed many millions. This has now developed the appearance of an uncontrolled pandemic. However, it had all the reasoning and information never to have become one. Was it ever really a pandemic? The panic and fear are real, but is the information used to create that fear and panic really all it is made out to be?
Right now, it is hard to rationalize what actions to take, but it is important to stop, think and realize that we need a better plan next time (and there will be a next time). This is now the fifth pandemic that is directly connected in just over two decades. This ignores many other global health threats that we have faced and overcome in the same time period.
We appear not to have learnt from how these previous pandemics were handled in the recent past. This is an occasion though where the saying, "Those who cannot remember the past are condemned to repeat it." (George Santayana), is ironically turned on its head. Instead of following the lessons of previous outbreaks, we triggered a worse case scenario plan.
There are people in the world from First Responders to Government to Armed Services, who will recognize the ‘break glass in case of emergency’ plan that has been implemented by Governments at all levels globally. However, this plan was never designed for what we are dealing with now. It was designed to deal with a global emergency of catastrophic proportions and with it came government powers that should never be taken lightly.
There are also professionals who deal with Business Continuity Planning (BCP) and Disaster Recovery Planning (DRP) who will recognize that this plan appears to have no nuances or layers. Those people understand that there can never be a ‘one size fits all’ for disaster planning.
Before we answer the first question, we must touch upon the second.
The real question is, “Is this virus worse?” The answer to that, as regards the virus itself, is NO. How can that be you ask? This has caused a global collapse the likes of which has never been seen before.
It is the reaction and impact to society that is worse, not the actual virus. This reaction is causing a feedback loop that is actually making the impact of the virus and loss of life worse. However, no-one is asking how many people (outside of COVID-19) are dying in hospital or waiting for treatment due to the stress these new protocols have placed on the system. People didn’t suddenly stop getting sick or requiring treatment for other just as deadly (and worse) ailments. Why are they being ignored?
The media says that regular flu has a mortality rate of 0.1% and COVID-19 is 2%-3%. That number for COVID-19 changes every day for each country from less than 0.1% to over 20%.
This study suggests that COVID-19 infection rates are already widespread which would put the mortality rate well below that of seasonal flu. Coronavirus may have infected half of UK population — Oxford study [Link]. This study also correlates with the massive, uncontrolled movement of people in and out of ground zero for months before countries went into partial lockdown. More recent studies on wider spread antibody testing suggest that even this Oxford study may underestimate the actual spread and therefore bring down the overall mortality rate below seasonal flu. This is backed up by the known and well-studied expectations of the spread of a highly infectious virus such as COVID 19.
Seasonal Flu
These are long term statistics gathered over decades. This does not come from testing every person who has flu though. This 0.1% number is also based on millions of people contracting the flu seasonally, despite over 50% of the population being inoculated (think the ultimate in self-isolation). By the definition we are using for COVID 19, the flu is a far more serious perpetual global pandemic! https://gis.cdc.gov/GRASP/Fluview/FluHospRates.html
COVID-19
These are rapidly changing numbers associated with testing people who appear to be symptomatic or who have had direct contact with a person who has tested positive. This assumes only the people exhibiting symptoms and being tested have it. Even with this, they know over 80% of people infected have minimal symptoms and recover with no issues. Further, more than 90% recover in this small sample group.
Extensive testing and new protocols impact the ability for the health system to deal with existing patients and other illnesses. Essential medical personnel are being redirected to full time testing. In the meantime, their regular work is handed off or shelved temporarily. Remember the health system is not dealing with just COVID-19.
Protocols have been escalated in health care to almost biowarfare levels, way beyond that of the protocols for far more deadly and infectious diseases. Unlike anything before, family members are separated at the doors of hospitals placing strain on health workers, family and the sick and dying. The strain this puts on the health system is creating a self-fulfilling prophecy. Have you ever been to a hospital treating MRSA (Methicillin-Resistant Staphylococcus Aureus), the ‘Super Bug’? Imagine that scaled to every aspect of the health system and then double it for the new protocols. Even without a single case of COVID-19, these protocols are unsustainable.
Now remember that this outbreak started in one of the most populous areas on the planet. It was highly contagious and had a long incubation period (before and after infection) with minimal to no symptoms. It started no later than mid November 2019 (maybe as early as August 2019 based on satellite and search data available at the time but only just released to the public) and travel was not restricted globally until almost 5 (to 8 1/2) months later. During that time, tens of millions of travelers moved in and out of that area at high levels due to Christmas, New Year, Chinese New Year etc.
How did China manage to keep the deaths to 4,633 out of 83,221 infections in a population of 1.4 Billon over a period of five months of reported outbreak in the region? Note that actual figures on testing are not available (as is most information on China).
hello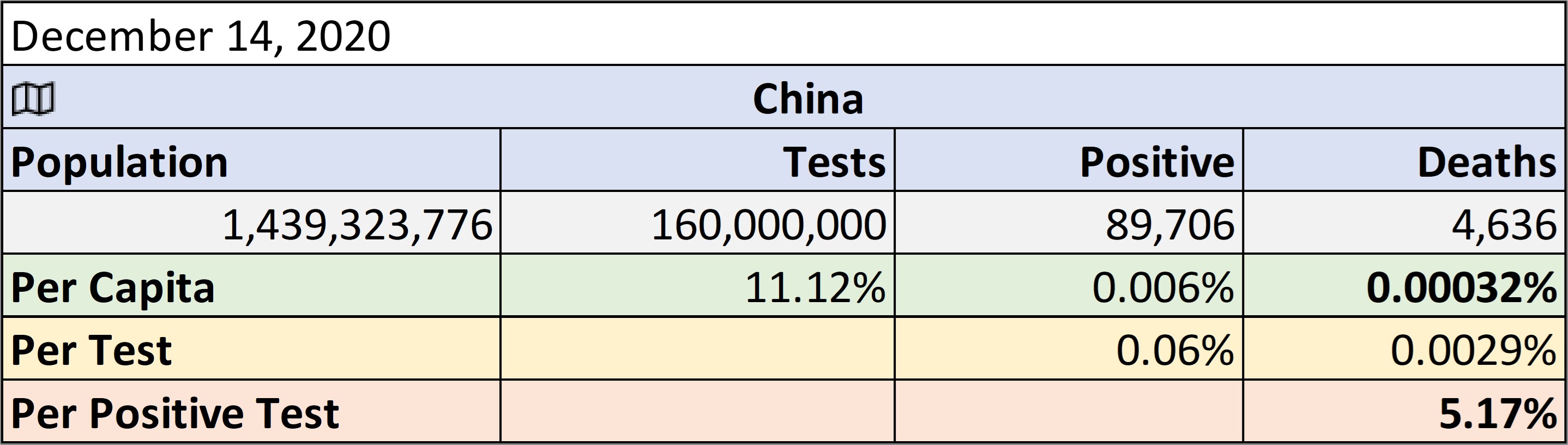 goodbye
goodbyeWith so few deaths, why did China need sixteen large temporary hospitals for such a long time, on top of their existing medical infrastructure? How many people moved in and out of that highly infected area in the months before the world locked down? Something doesn’t add up.
Anyone who understands statistics will see a few glaring issues with what is currently being reported.
The CDC just published seasonal flu stats for the US. Up to 56 million infected and up to 62,000 deaths in the same November to April period. https://www.cdc.gov/flu/about/burden/preliminary-in-season-estimates.htm.
Why is this relevant?
Flu transmission is controlled by a large number of the population being inoculated. The spread of flu has been controlled this season by the exact same steps as those implemented for COVID 19. However, it still killed up to 63,000 people in the US alone in the same 2019/2020 period as COVID-19.
As testing increases for COVID-19, the numbers continue to change. More people appear to have contracted COVID-19 daily, or have they? More people are tested daily as tests roll out. Testing turn-around time has been reduced from 6 days to 15 minutes or less, so we see another spike in reported cases. This doesn’t mean COVID-19 is necessarily growing exponentially despite the numbers growing as testing increases.
We need to be careful when referring to the terms 'Cases' and 'Confirmed Deaths' as they do not mean what many people think. As such, they, should be used with caution (unlike John Hopkins University, Bing COVID 10 map, The mainstream media (MSM) and daily government updates). Note: The actual definitions and criteria are available from the CDC, WHO and many Government sources (as is shown in these articles and links).
As of April 29th, 2020, the Canadian Medical Association Journal (CMAJ) guidelines state that COVID 19 has an overall mortality rate in tested positive cases as 0.1% (1 in 1000) [Link]. CMAJ quote this low mortality rate as a reason not to use any proven safe, cheap and effective medications for the treatment of mild to moderate cases. For COVID 19 (SARS-CoV-2) we are using a confusing mechanism in a clear attempt to artificially inflate the presumed actual mortality rate of the virus i.e. risk of death. All reporting now uses [Positive] ‘Case Fatality Rate’ (CFR) as an indicator of how likely it is for you to die of COVID 19. However, this is the percentage of the tested (not currently infected or recovered) positive cases. This is the ‘numerator’ (the number at the top of the equation). This is placed over the number of deaths presumed to also include COVID 19. Note this isn’t a death were COVID 19 is the primary cause or primary contributory factor in the death. In fact, it isn’t even something that may have been tested for and is, as per CDC guidelines, acceptable to assume COVID 19 in some cases. This then forms a very questionable ‘denominator’ in the equation. We are therefore reporting the most significant piece of information ever reported in the history of the world based on two very questionable numbers.
A true risk of mortality (as calculated in every other pandemic is the actual rate of infection (number of people who caught the disease) over the people who actually died of the disease. This is a much lower number than is being reported.
'Cases' are not the spread of the virus, but rather the targeted testing of a grouping of people expected to test positive. This has been consistently around 20% in the US. As this is targeted testing, the low rate of positive numbers in a group expected to be positive should be worrying. However, this results in a lower numerator (‘Cases’) which will increase the mortality percentage. This would not normally be an issue if you know how the numbers are derived, but many don't.
The denominator ('Deaths') are, as per the WHO and CDC guidelines, any person with or suspected of having COVID 19, where COVID 19 may have been a contributing factor. As there are many contributory causes of death, this number must not be assumed to be the only or primary cause of death. However, this is not clear in most reporting. Clarity is critical when you consider the impact of the decisions being taken in this scenario worldwide.
When misused as a reason to close the world, putting many lives in jeopardy from the consequences of a global lockdown, this is beyond negligent. It constitutes a crime against humanity!
As an analogy to how these numbers are being reported, let's consider the way that governments justify everyone's favourite selfie moment, 'Photo Radar' for speeding.
That being said, it is likely the numbers are growing. Sadly, partial self-isolation may be making the situation worse not better. We have taken a population with an unknown but likely high infection risk and partially isolated them. Inside these family or social isolation ‘pods’, ‘social distancing’ does not exist. If one person contracts the virus, all are likely to be infected. This isolation has increased stress, reduced time outdoors, created an unhealthy and sedentary lifestyle, all leading to many avoidable risks to our physical and mental health. As such the impact of this unnecessary lockdown will be felt for decades, if not generations to come.
We have allowed one or more mombers of these ‘pods’ of people to go to small, concentrated and now more heavily frequented locations such as grocery stores, gas stations and fast food drive throughs. Each of these locations has a number of common use hard surfaces made of plastic and metal that we handle without a thought. This isn’t just about COVID-19. Gas pump handles for example are as filthy as a toilet seat (https://www.reuters.com/article/us-usa-health-filth/gas-pump-handles-top-study-of-filthy-surfaces-idUSTRE79O0G820111025). As COVID-19 is primarily transmitted by droplets from our breath (coughing, sneezing and even just breathing in some cases), it is these commonly handled surfaces that pose a potential risk of infection. These locations are not cleaned between visitors as an operating theatre would be.
Although no specific cases of hard surface transfer have been cited yet, it is a known risk for virus and other communicable disease transfer in general. Every hard surface can hold the virus for up to 4-5 days (or much longer).
"SARS-CoV-2 RNA was identified on a variety of surfaces in cabins of both symptomatic and asymptomatic infected passengers up to 17 days after cabins were vacated"
https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e3.htm
Soft surfaces 1-2 days. None of these surfaces, outside the health system, are being regularly or appropriately disinfected. There are a growing number of cases with no apparent source which could easily be common surface transfer cases. Further, in studies, COVID 19 has even been found to be stable in the air for 3 hours or more.
Doctor Marc G. Wathelet, the distinguished virologist in charge of a team studying SARS.
"An aerosol, literally a solution in air, consists of micro-droplets, which are so small that they stay suspended in the air or fall much slower than small droplets. They are produced during normal breathing and this production is accelerated by speaking or even more by singing, shouting."
"The presence of more cases where the first symptoms are pulmonary for COVID-19 is a clear indication that transmission also occurs by aerosol."
https://www.paulcraigroberts.org/2020/03/09/covid-19-and-aerosol-transmission-some-thoughts/
https://www.nejm.org/doi/full/10.1056/NEJMc2004973
All the data seems to suggest that COVID 19, while highly infectious, is relatively low risk for all but the most vulnerable in society. Yet we have locked up everyone. This was a necessary part of the plan that was triggered, but is criminal to have been misused as it has been.
As transmissible by fomites (hard surfaces such as water bottles) or direct contact (mucous membranes) and being airborne, COVID 19 qualifies as a “High consequence infectious diseases (HCID)” in the UK. In fact, it was classified as such until four days before their lockdown.
Four days BEFORE the UK locked down it declassified COVID 19 as a High consequence infectious diseases (HCID) because [link];
"...more information is available about mortality rates (low overall)…"
Since the lockdown in the UK, COVID 19 has been found to be orders of magnitude less deadly than it was thought even then. Yet the lockdown continues worldwide.
Why is that?
What is listed as a HCID is;
*Note that SARS-CoV-1 (the original SARS) is on this list and yet there hasn't been a case since 2004. There is also NO vaccine** for the original SARS*.
**The common cold is a coronavirus (OC43). Coronaviruses account for 10%-30% of respiratory infections worldwide (as per Dr. Fauci) but have never locked down the world. https://www.cdc.gov/coronavirus/types.html
There has never been a vaccine created for any human coronavirus; https://www.cdc.gov/coronavirus/general-information.html
Less than 2,000 'cases' (not 'deaths') in China alone, & drug makers 'rushed' to create a vaccine. This, despite no-one ever developing such a vaccine before. A cure for the common cold - Woo Hoo (or is that Wuhan). 50 years trying with no success for any coronavirus!
Jan 23 2020. https://www.wsj.com/articles/drugmakers-rush-to-develop-vaccines-against-china-virus-11579813026
Canada clamoring to cure the new ‘common cold’. https://globalnews.ca/news/6466954/coronavirus-outbreak-vaccine-research/
Thanks Dr. Fauci for suddenly jumping on the vaccine money train. Maybe you will cure the common cold as well!!! https://jamanetwork.com/journals/jama/fullarticle/2759815
We should stop comparing COVID 19 to the flu as H1N1 etc. have a vaccine.
COVID 19 - the new & improved 'Common Cold'. What is this really all about?**
No other country (outside of China) has ever locked down its healthy citizens for any of these more deadly highly infectious diseases. So, why have we locked down the world for COVID 19?
In our new isolated way of life, we touch the same gas pump, shopping trolley or pay terminal (and more). The users and operators of these locations are not sanitizing (gloved or ungloved) between every surface touched. How is this controlling the spread and enforcing isolation? In effect, it is merely giving the appearance of isolation and control.
In fact, grocery stores have now decided that single use bags are a transmission risk. We have moved from banning single use plastic bags to not allowing re-usable bags. How times change in such a short period. In Alberta, the initial spread of infection coincided with most grocery stores banning single use plastic and requiring re-usable bags.
Each of the designated shoppers now come back to their family pods with an increased likelihood of exposure putting at risk the very people they are striving to protect.
This example touches on three ‘essential services’ that our partial isolation puts us in direct contact with daily. None of these are running with biohazard protocols.
Recently, the Government of Ontario published a list of 74 groups of essential services. It is hard to find a service that doesn’t fall into one of these 74 categories. How many people are now moving in and out of high infection risk areas each day?
This might explain how Italy deteriorated so quickly when they went into partial isolation first. Note that there is no such thing as full isolation that does not result in many more deaths. The only full isolation is in a plastic bubble in a hospital. Think of the movie ‘The Boy in the Plastic Bubble’ starring John Travolta. That is not possible with a population needing food, medicine and any of the other basics of today’s life. Additionally, northern Italians have an apparent genetic trait that increases the impact of an infection such as COVID-19 (https://www.ncbi.nlm.nih.gov/pubmed/18603552). As of April 11th, 2020, most of the cases in Italy are still focused in the northern region. Out of 17,127 deaths in Italy, only 1,083 have been in southern Italy. In addition, they have one of the oldest average populations in the world.
The late notice of the disease and increased global travel within China in recent years allowed the virus to spread throughout the world unchecked. China’s borders have not been as relaxed as in recent years, so previous spread may have been more contained. Secondly, the prior outbreaks were managed through regular infectious disease protocols (not global lockdowns). Lastly, prior outbreaks were treated with a known prophylactic and treatment at the time. Effects of chloroquine on viral infections: an old drug against today's diseases [Link]. This is the very same medication and treatment protocol suddenly being tentatively ‘trialed’ by doctors and questioned daily by the media. The use of Hydroxychloroquine along with anti-biotics is not a new miracle cure for a Coronavirus such as COVID-19. It was used to treat Avian Flu (1997), SARS (2003), MERS (2012-2015) and many other diseases that cause a cytokine storm (such as lupus) for decades. This is why Australia, France, Canada the US and many others are now testing it. As of April 11th, 2020, WHO are apparently expanding testing globally for this decades old drug. However, the obvious push back on this drug, but not others is noticeable.
One question must therefore be asked. Why did it take it taken five months, over twenty one thousand confirmed deaths (by April 11th, 2020) and a global economic meltdown before this was openly discussed and used to save lives? Why are the FDA suddenly suggesting it is dangerous and should not be used, only in the case of COVID 19? Why is it now being shut down in favour of riskier untested and expensive treatments? [Link]
It is a drug that was invented in 1934 and has been used to treat malaria, lupus and rheumatoid arthritis for many decades. It is cheap, freely available and even the manufacturers are offering millions of free doses to get through this crisis. This is something Governments have been ignoring until one world leader, The US President, Donald J. Trump, pushed back. He forced the FDA to allow the drug to be used, which, up to that point, was apparently being held back by red tape. Whether you love or loath President Trump, we are now seeing the dam break. Global testing is now in full swing.
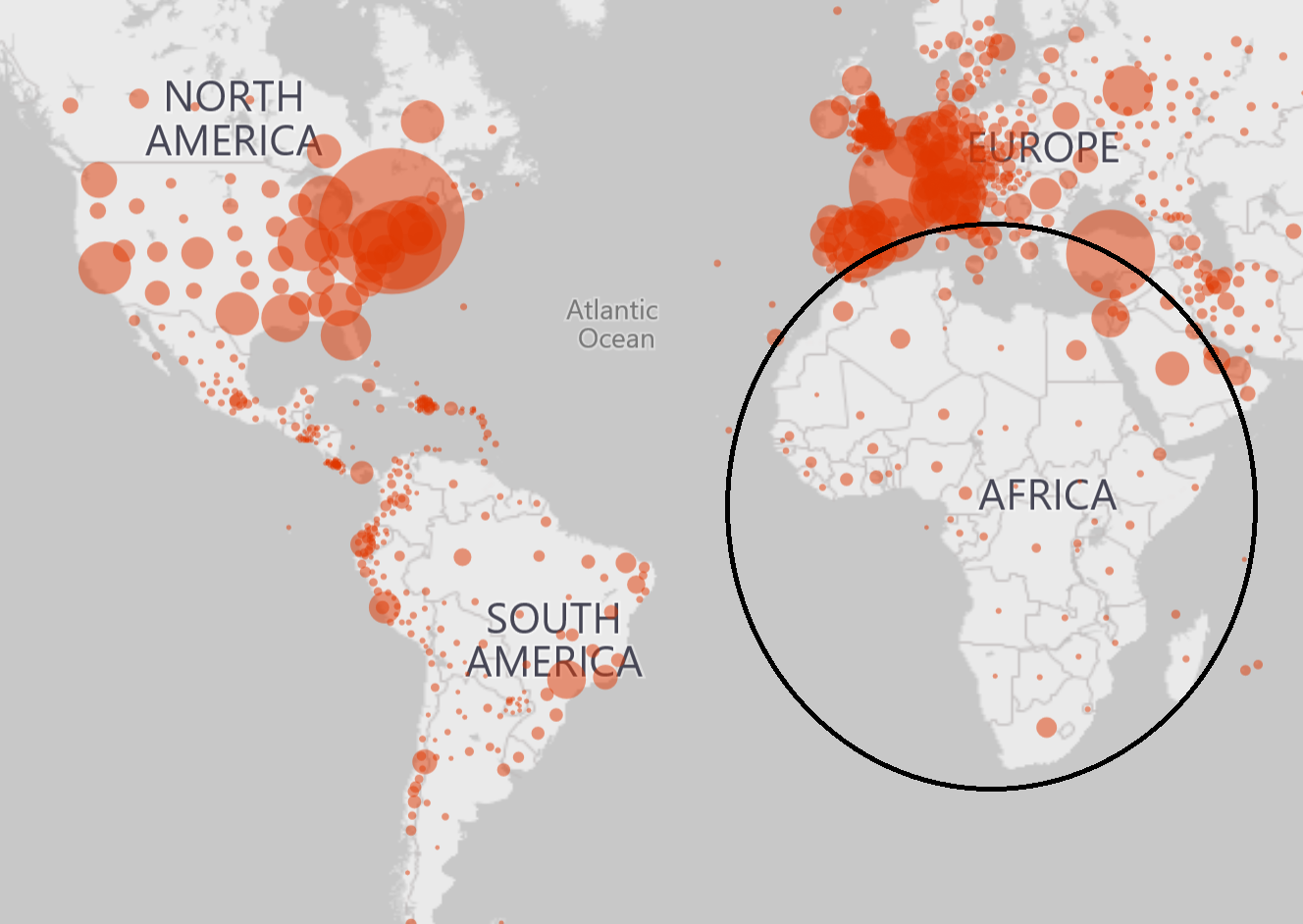
Speaking of malaria. Take a look at the malaria world maps and overlay the coronavirus maps. It is interesting to compare the areas of COVID-19 and malaria prone countries.
Although there are pockets of COVID-19 in areas with malaria, the incidence is very small in comparison to the surrounding countries. Africa, for instance, has a population of 1.3 billion. As of April 11th, 2020, Africa had 412 deaths and 9,079 confirmed cases out of 1.3 Billion people. Of that, 40% of the reported cases came from one areas in a tight cluster, Egypt, Tunisia and Algeria. If there were no incidences reported, it would suggest a lack of data as not everyone is taking the medication all the time.
What makes Africa so different from Italy and its 60 Million population with over 17,127 deaths and over 135,586 infections in 45 days from the first reported death?
https://www.treated.com/malaria/world-map-risk
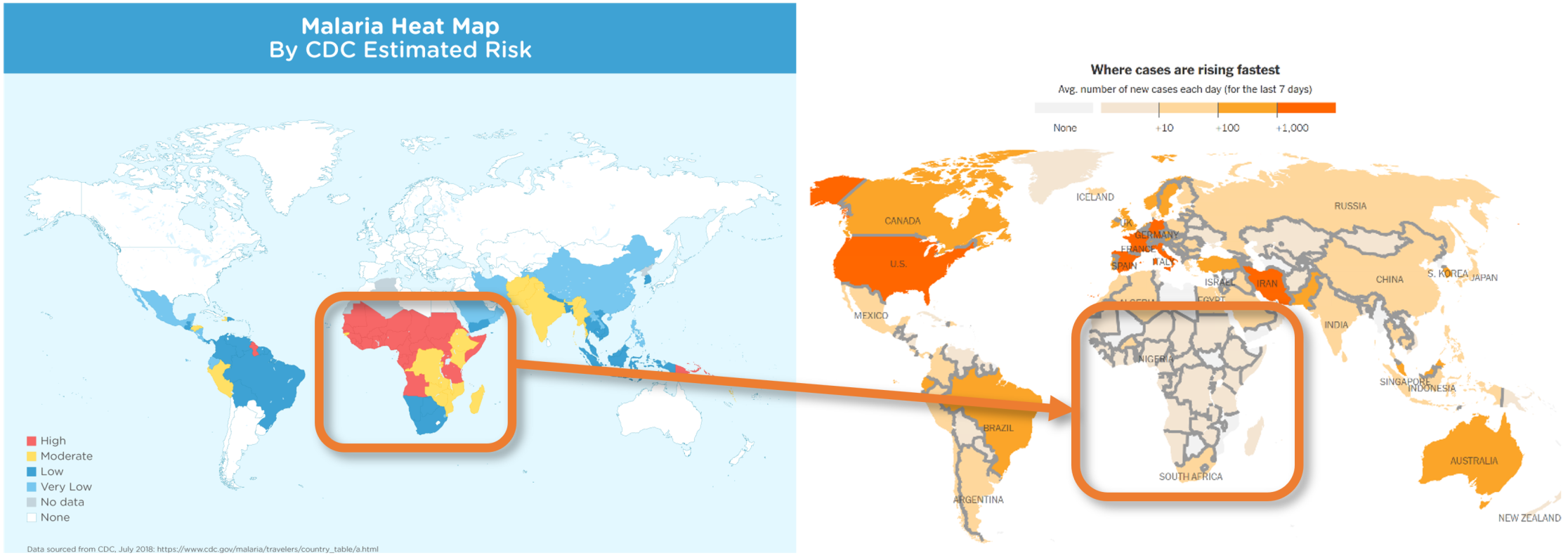
In these maps, we see two things.
Lack of travel/population and high risk of malaria coincide with low numbers of infection and mortality. Is this really just a coincidence?
What about the spread of COVID 19. Here is the map of the COVID 19 spread as of April 19th, 2020.
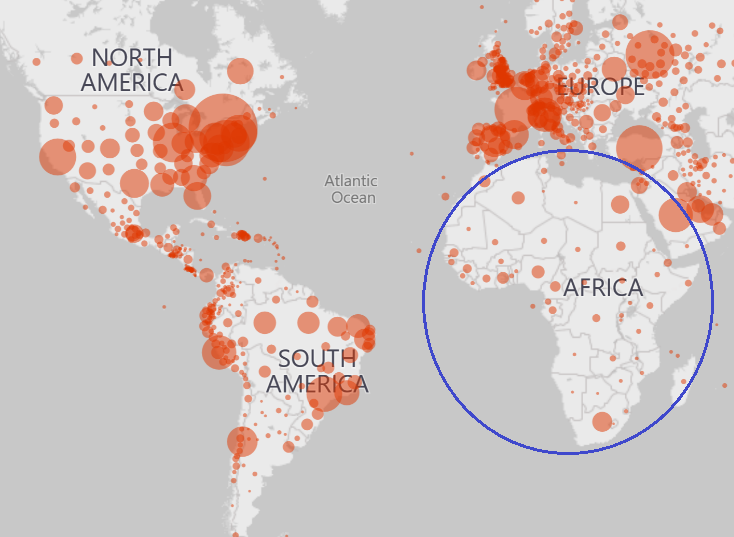
Here is the same map of the COVID 19 spread as of May 28th, 2020.
Countries have implemented the only global disaster plan they have. It was designed for nuclear war and similar global scenarios where deaths were guaranteed in the millions. We have essentially implemented globally a ‘break the glass’ plan where the expectation is casualties and deaths due to the extreme nature of the crisis. The plan is designed to deal with an incident that would kill millions, so 'the casualties of war' position makes sense. This plan was never designed to deal with the type of scenario we are now facing.
We need another plan!
Controlling the population was critical in the plan for nuclear war. That can only be achieved if the population is contained. There are not enough Police or Armed Forces to contain a moving population. In prisons, guards don’t try and control prisoners in the exercise yard. They lock them down. It takes a lot less manpower to control a population that is already contained.
Why did Governments across the globe implement their ‘break the glass’ plan? Because it is the only one they had. The larger question is why did they implement this plan this time and not before?
For SARS and MERS, countries quickly implemented localized infectious disease protocols. They also started the use of anti-malaria and other drugs early. Information globally was sparse and both travel and communication in and out of ground zero (China) was limited.
China tightly controls information flow in and out of their country. In past outbreaks, the Chinese reaction remained hidden from sight. This time, the information coming out of China due to global communications, social media etc. fed into panic protocols being implemented, one Government after the next. One Government (China) implemented this process, let other Governments observe it and boom, everyone is metaphorically ‘panic buying toilet paper’. The mentality is, right or wrong, ‘we can't be blamed for doing what everyone else does’.
Back to the comments on a DRP and BCP. Organizations from small business to Governments sadly ignore these plans and very rarely update them. The belief is what they plan for doesn’t ‘normally’ happen!
Yet, disasters do happen. These plans have to be living documents with layers for many scenarios. When the current global threat plans were created in the 60's-80's, there was only one scenario to plan for 'Global Thermonuclear War'. That risk still exists (with North Korea, China, Iran etc.), but now there are other risks, from 9/11 to the 2008 financial collapse, to SARS, MERS, H1N1, H5N1 etc.
We need a better Plan!
This exact scenario wasn't just predicable; it has happened four times already in just over two decades (SARS, MERS, H1N1, H5N1). Yet, the people who advise Government and manage these plans either did nothing or were not heard. Most of the lack of action and planning, as we know, is due to budgets and the mentality of ‘BCP/DRP, what's that?’. This has to change.
We need a better Plan!
The only hope is to learn from this. It is a fact that “those who fail to plan, plan to fail”. Or as DNA (Douglas Noel Adams) said,
“Human beings, who are almost unique in having the ability to learn from the experience of others, are also remarkable for their apparent disinclination to do so.”
What is the answer right now? The world has gained momentum. We are on a course where it is hard to slow down and almost impossible to stop. The iceberg is here, the Titanic is sinking and we do not have enough boats (or ventilators, doctors, nurses or beds).
However, this is not 1912. We have more lifeboats coming along with every resource available to us. The Hydroxychloroquine trials are a start, as long as the media’s worry mongering doesn’t scupper the plans. Already we have the media blaming the US president for three people in Nigeria overdosing on an over the counter drug! They also blamed him for a couple taking Chloroquine Phosphate from their aquarium supplies, despite it being clearly not for human consumption. Why did the media not blame the Australian, French and US researchers that published the information in the first place? If the US President said Acetaminophen was good for headaches, would he be blamed for the many overdoses that happen every day? People have said if Donald J. Trump found the cure for cancer, people would ask why it took so long. I guess they were right.
We have to learn from this. We have to change our response to this type of crisis in the future. This will happen again.
We need a better Plan!
“Shame me once, shame on you, shame me twice, shame on me…”
In just over 20 years alone, we are now up to five!!! Shame on everyone if we do not learn and adapt our plans this time.
Maybe next time we need to stop, think and ask;
We can't blame anyone right now. This is not the time for the distraction of a postmortem deep dive looking for blame. There will plenty of time for that, if we survive the current plan. The body (the human race), is still warm and breathing unassisted. We are slowly being smothered though. So, for humanity’s sake, we have to learn from this tragedy. We didn’t devolve into panic with SARS, MERS, H1N1 and H5N1 some of which, show higher mortality rates.
We need a better Plan!
In the current crisis, we have an apparent abundance of information. Yet are we really seeing the true story? Right now, the facts being presented are based on targeted testing of likely ‘Positive Cases’ to misleadingly demonstrate inflated mortality rates. Typically, mortality rates are based on per capita or widespread random sample numbers.
We are continually being told we need to flatten the curve. However, the curve can be artificially manipulated when the figures are based on the number of tests performed and CDC guidelines have almost eradicated any other cause of death.
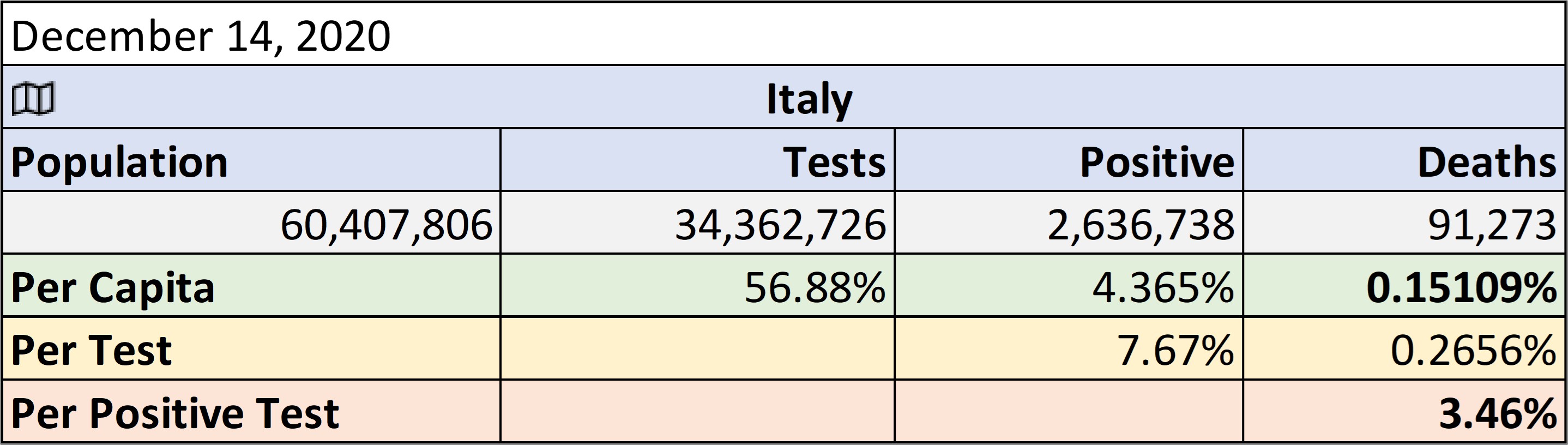
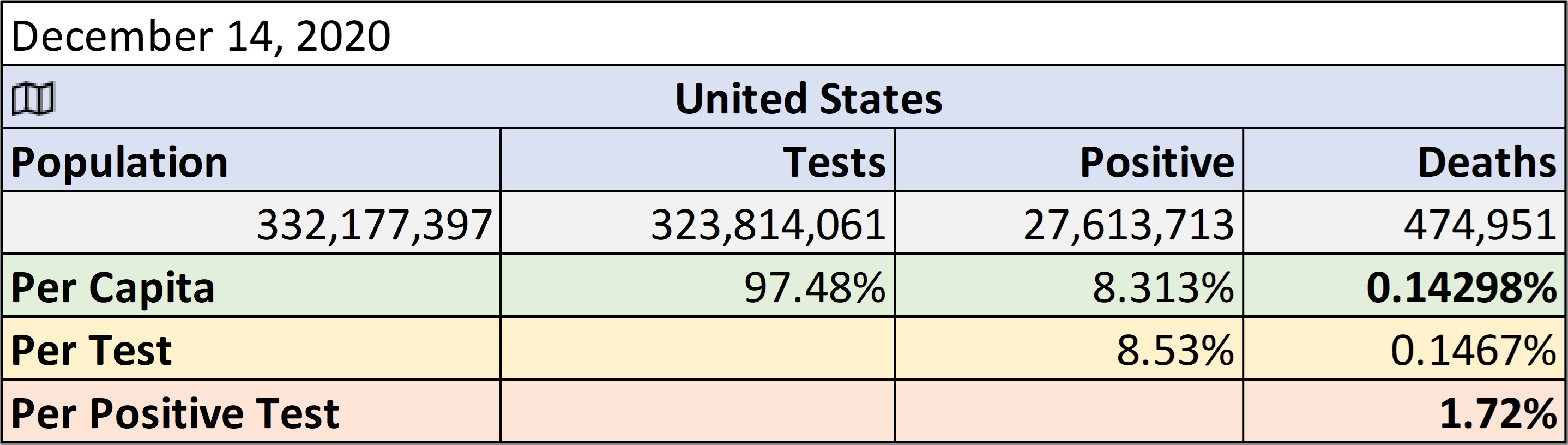
The US and Italy are prime examples of this misinformation. It should be noted that due to an aging population and other factors, Italy has one of the world’s highest mortality (death) rates from seasonal flu in the world.
Based on this, you are 50% more likely to catch flu in the US than Italy. However, you are 600% more likely to die of flu in Italy than the US. Maybe the death rate from COVID-19 in Italy makes sense after all.
(https://www.sciencedirect.com/science/article/pii/S1201971219303285).
As on the beginning of April, 6 weeks into their full lockdown, Italy had a reported mortality rate (deaths) for COVID-19, per active case, of about 19.42%. This is the number used to frighten the population. But this is a number with no value whatsoever, other than to induce fear. If you are only looking for horses, you will never find a zebra, even if it is there. If you only test those most likely to have COVID 19, what else would you expect to find?
Digging deeper, ( https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geographic-distribution-covid-19-cases-worldwide) we find that deaths per tested individual is 0.73%, down from an avaerage of 1.4% before anti body testing. However, this is another number with minimal value as testing is on those most likely to have caught COVID-19. The likelihood of death should be based on the per capita number in absence of widespread random sample testing. As of June 16th, 2020, the mortality rate in Italy was 0.057%. That is the only supportable statistic to show the actual chance of dying right now. Italy's mortality rate is something above but closer to 0.057%, not up to 20% (or 14.49% as of June 16th, 2020) as the media and others have pushed.
For the same day in the US, well into the 'social distancing' and lock downs, these numbers were 5.41% based on positive tests. For each person tested, it was 0.47%. However, per capita, the unreported rate was 0.036%. You can’t control a population with those numbers though. So, the media pushes the escalating positive test results as if people are catching it at this same escalated rate with a false mortality of 5.41% at that time. In other locations around the world (as we move through each area), we see similar numbers. Again, the push is on the skewed numbers that cause panic.
Even here the reported numbers by the CDC themselves depend on what page you look at;
The main splash page for COVID 19 from the CDC showed 62,406 deaths as of May 2nd, 2020. Interesting that this is the figure the press, John Hopkins, Bing and government report. https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
Then there is the Respiratory disease reporting page with flu, COVID and all cause mortality based on provisional death certificates (the most accurate data) that showed 37,308 deaths 'from' COVID19 on May 2nd, 2020. https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
To make this worse, the 37K deaths are combined with other causes of death, plus not necessarily confirmed to even have COVID 19.
"Deaths with confirmed or presumed COVID-19, coded to ICD–10 code U07.1"
This artificial inflation of the 'death' count is by design and according to CDC and WHO directives.
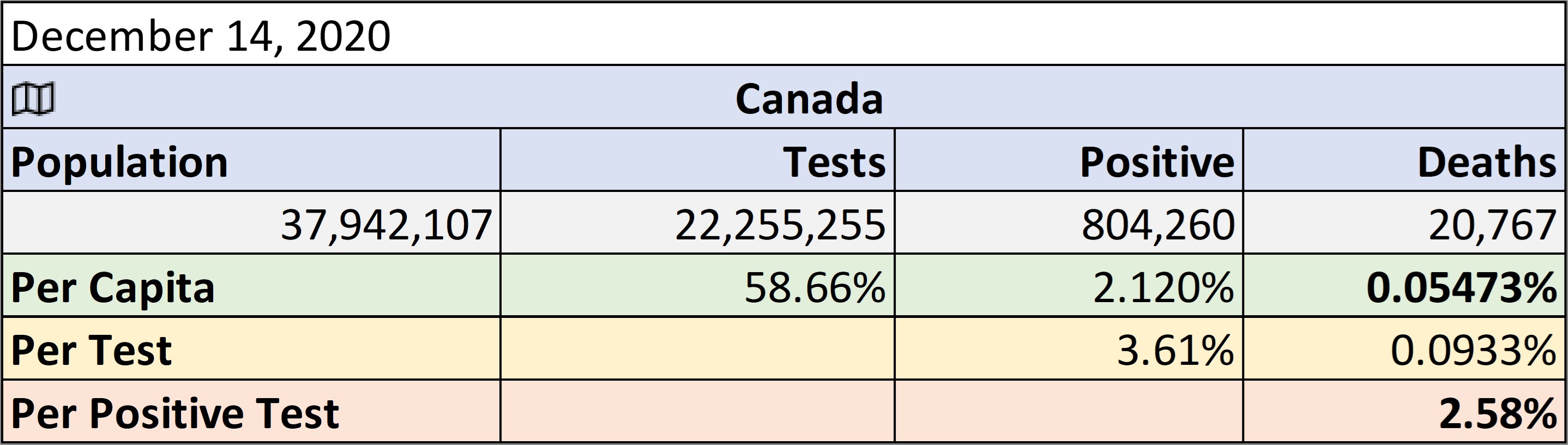
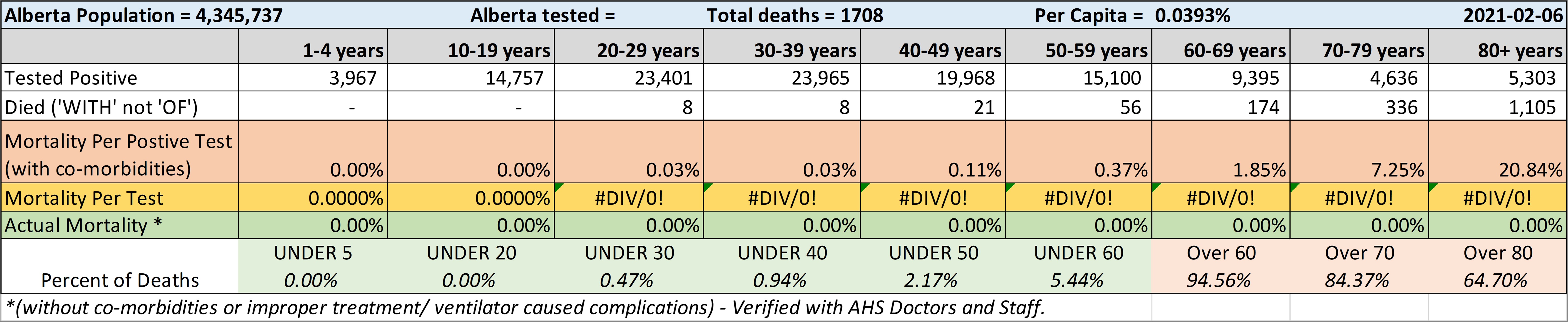
Alberta in detail.
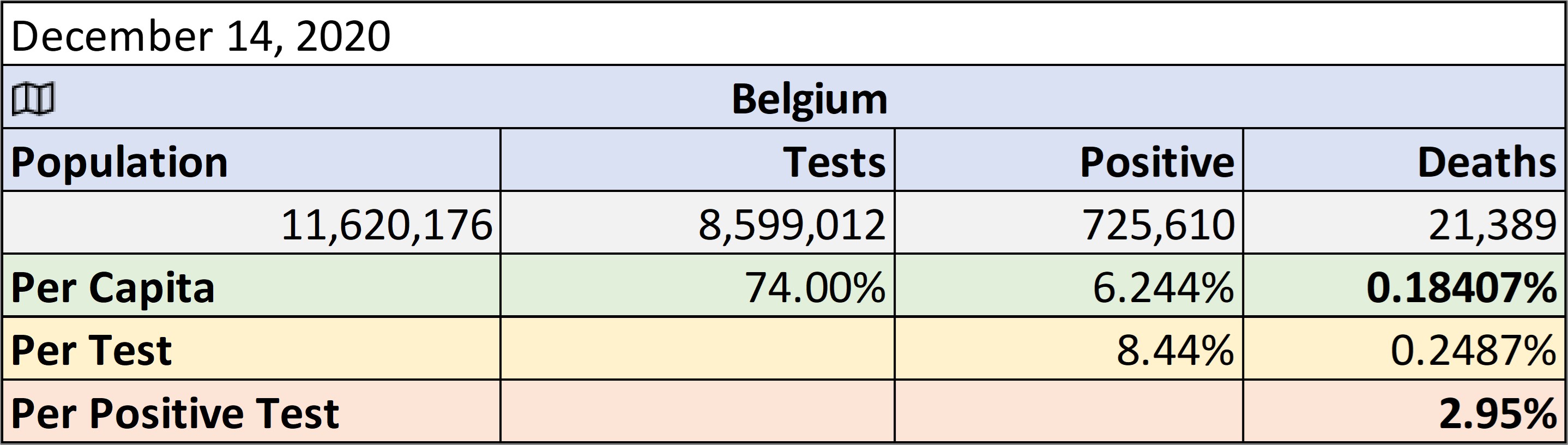
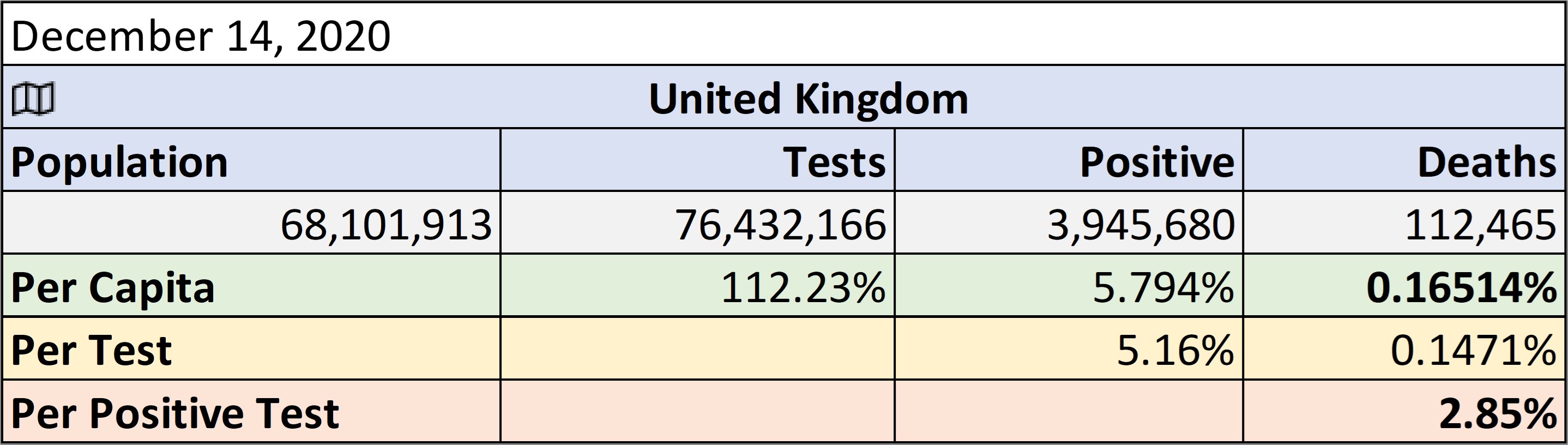
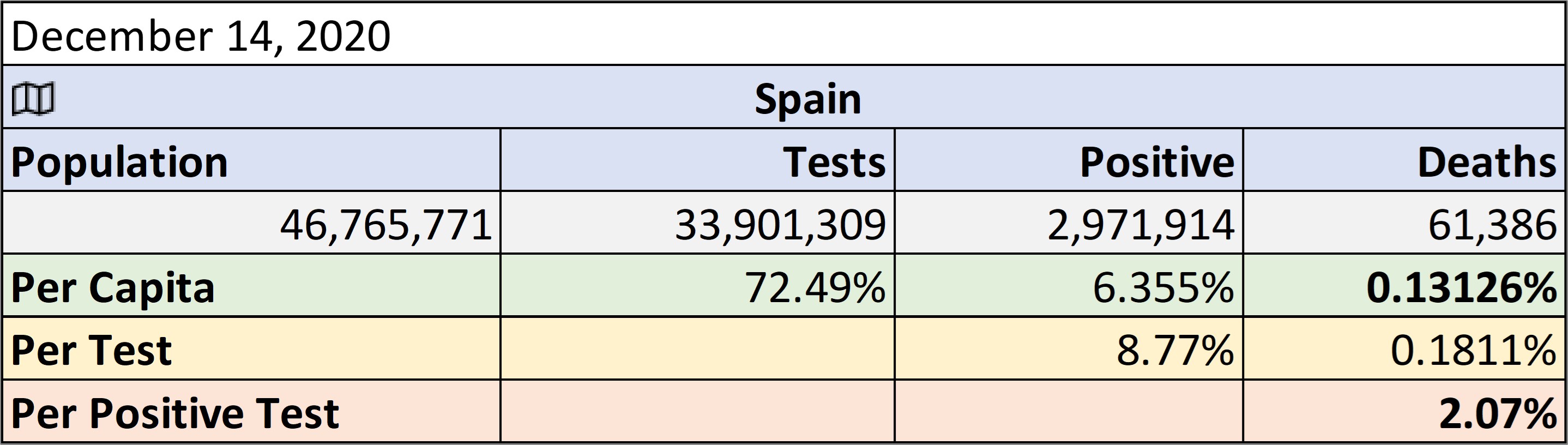
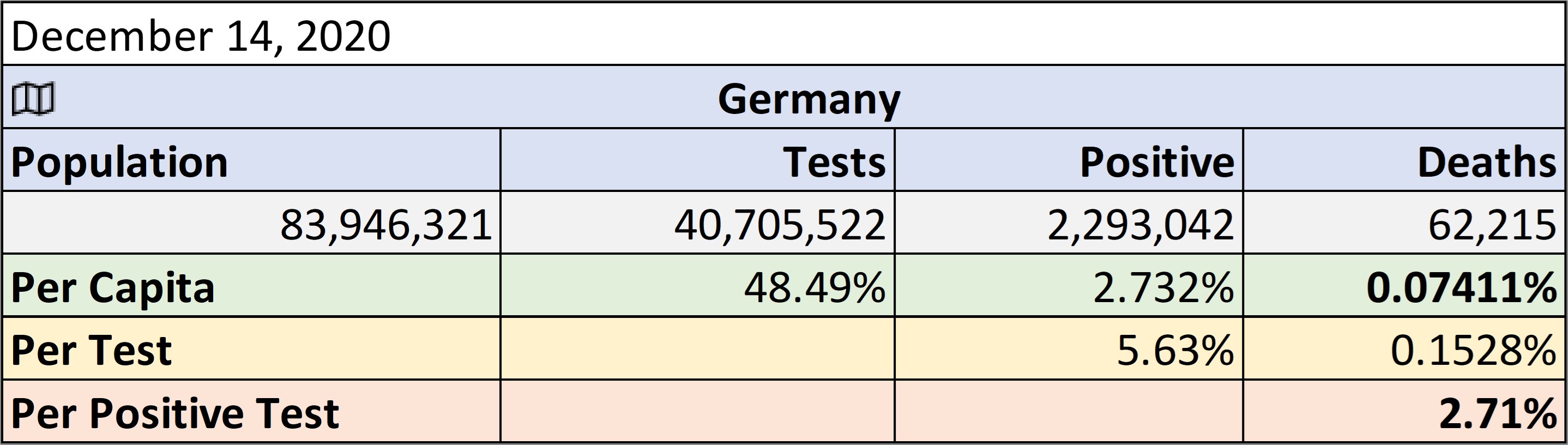
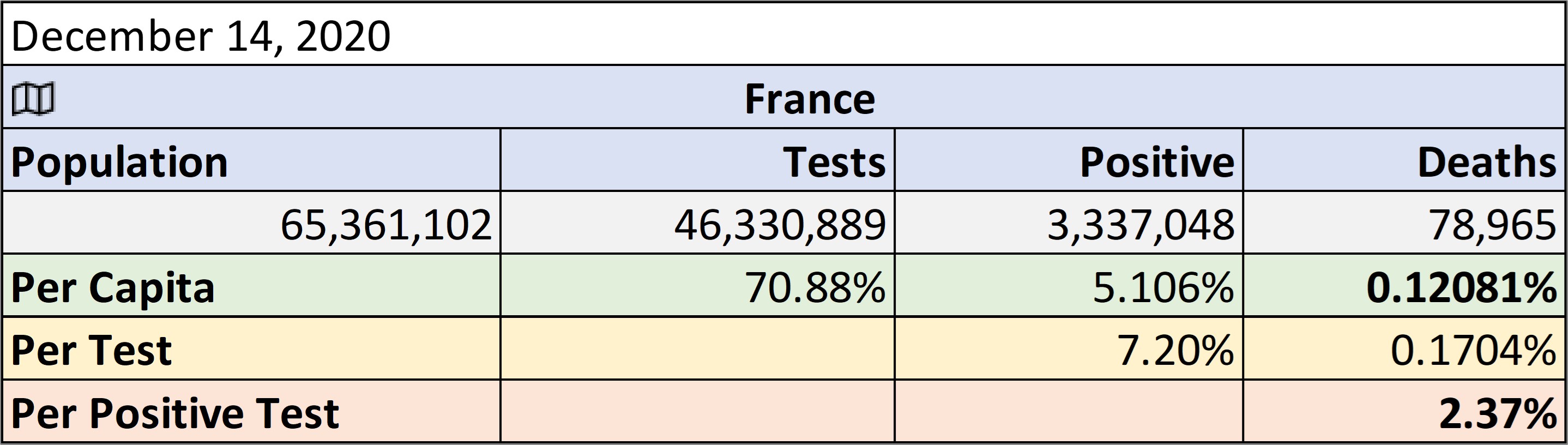
Notice how the ‘Mortality’ rate being reported (per positive test, not per capita) is widely changing daily (up and down). Notice how it does not align between any country, even though that share similar demographics such as the Scandinavian countries. As of June 16th, 2020, you are apparently 50% more likely to die of COVID 19 in Sweden than Switzerland (down from an average 2 times). But the per capita rate of mortality is statistically so close as to make no difference. Are you really 50% to 200% more likely to die in Sweden of COVID 19?
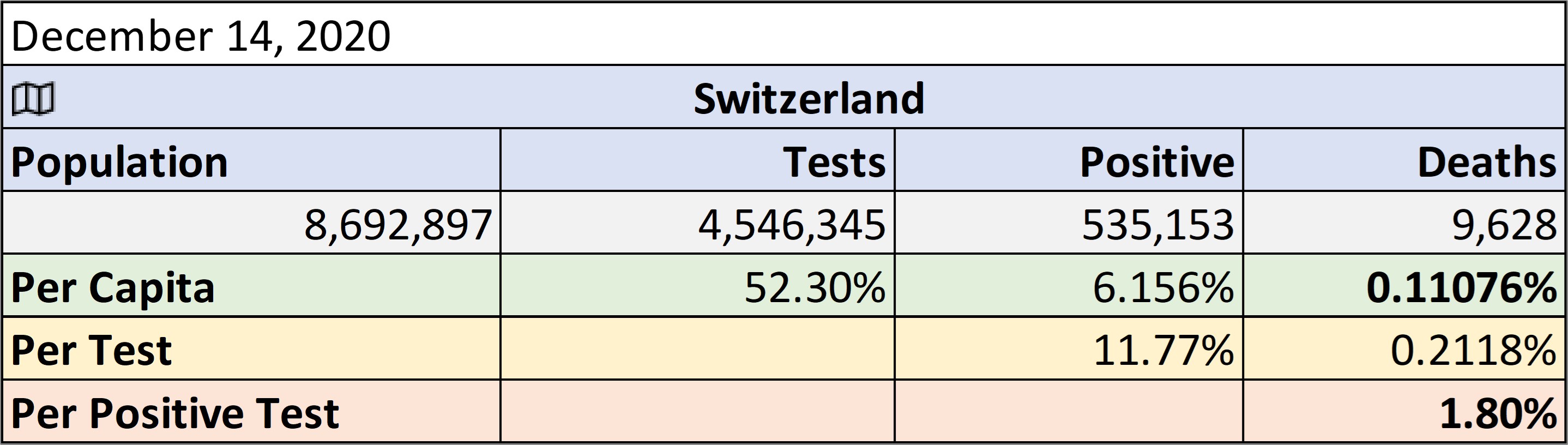
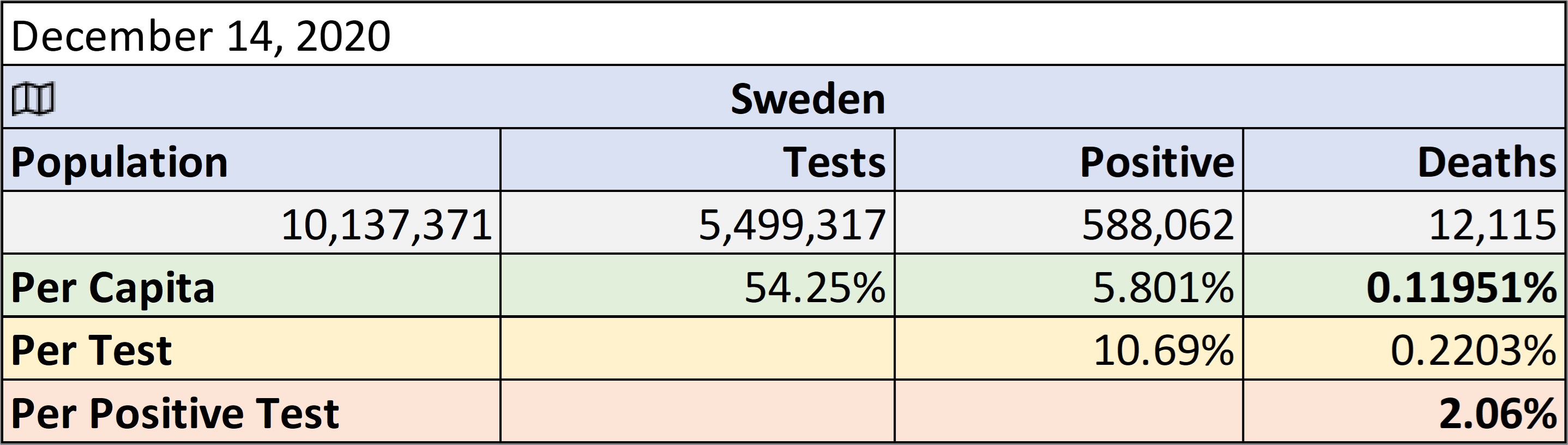
Add in Norway to this mix and you have half the population of Sweden but apparently less than a 1/3 chance of dying in Norway than Sweden. In the per capita testing that number becomes an order of magnitude lower. Sweden has had over 20 times more reported deaths than Norway. Switzerland, just over 8 times the deaths.
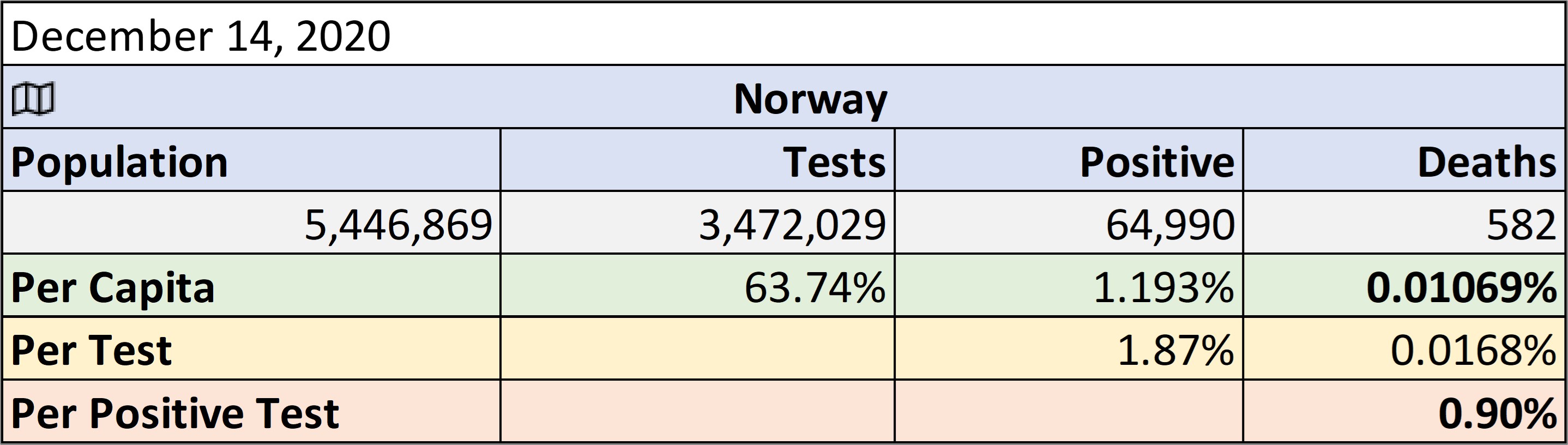
Yet, the regular life expectancy of all three countries is almost identical. In Norway that life expectancy is about 83 years old. The median age of a COVID 19 death in Norway as of June 16th, 2020 is 83 years old. Also note that the reported COVID 19 deaths on June 16th, 2020 for Norway was 293 on the John Hopkins and Bing Maps. However, the only official source of data for Norway comes from the National Institute of Public Health (NIPH), where the actual number is 242. (https://www.fhi.no/en/id/infectious-diseases/coronavirus/daily-reports/daily-reports-COVID19/).
In other locations around the world (as we move through each area), we see similar numbers. Again, the push is on the skewed numbers that cause panic.
Lies, damn lies and statistics at their best.
Have world leaders been fed these apparent false narratives? Is the US president the only one that might be seeing through them? Is this an explanation for the push to get back to work by him, and him alone? Or is this just a reaction based on a panic implementation of the only plan they had?
WE NEED A BETTER PLAN!
As the media fiddles, we are watching Rome burn. Only China appears ready to rise from the ashes. So, don't be a Nero. Join the conversation beyond the four corners of your TV and help us climb out of this hole before it is too late. #COVID19, #RomeIsBurning, #ABetterPlan, #jointheconversation
Now back to your regularly scheduled 'programming' update. Welcome to Stepford, 1984 style. How a to program a population to accept the 'new normal'.
Remember to eat your Soylent Greens.